Suggested, partial, initial, draft of a future FLCCC Vitamin D Supplementation Protocol
Robin Whittle rw@firstpr.com.au 2024-10-10 (#2024-10-17 update to my notes near the end, on 5000 IU vitamin D3 a day precipitating heart arrhythmias.)
Daylesford, Victoria, Australia +61 3 5348 4794
For Dr Marik and Dr Dalgleish
(printed) and all other FLCCC doctors and team members. This is
also written for Prof. Sunil Wimalawansa in New Jersey and Bill Grant
PhD in San Francisco who I hope will want to work on a Vitamin D3
Supplementation Protocol along the lines of what have written.
This is a private web page which is not linked to from any
site. In addition to reading the printed version, please
use your browser at:
to read this page
https://5nn.info/private/dp/1-protocol/ so you can follow the reference links to the References section, which contains links to the cited articles.
I will, but have not yet, write some notes on how vitamin D3 supplementation is referred to in the current FLCCC protocols:
There are some problems with the current material, including a
misleading diagram in the Cancer Monograph, this monograph not
addressing the problem of hypercalcemia in malignancy, and the Sepsis
protocol, where calcifediol or loading dose vitamin D3 is most urgently
needed, not mentioning vitamin D at all.
Notes in purple:
I propose that all the other FLCCC protocols, guidance documents and the
Cancer Monograph be rewritten to refer the reader directly to this proposed Vitamin D3 Supplementation Protocol
regarding long-supplementation and emergency 25(OH)D repletion with
calcifediol or a loading dose of vitamin D3.
These other protocols may elaborate on the core material below - especially
the Cancer Monograph, concerning the potential problems of
hypercalcemia in certain types of cancer.
Since the Cancer Monograph is intended to be a standalone document, it
may be best to include this Vitamin D protocol, the summary, or a
specially adapted version of these in the Cancer Monograph itself, or as
an appendix.
If you send me an example Word file from which one of
the Protocol PDFs were made, I can get all this text into that format,
with the right paragraph styles - and you can work on it from
there. I would leave the
references in their current form, since you will need to get them into
your own Zotero or Mendeley
databases to produce the final document.
Ideally, all the references in FLCCC protocols would include
clickable links. Without such links, as they are now, very few
people will have the time or patience to actually read the
references, such as by copying and pasting some text into Google Scholar.
This is all written freshly - not copied from my sites https://vitamindstopscovid.info or https://nutritionmatters.substack.com.
There's no need to credit me, since I have no academic qualifications
or research experience. I intend that the final document be
improved and approved by Sunil, Bill and perhaps other long-time
vitamin D researchers, who should be credited.
Ideally the FLCCC would not need to write anything like
this. You should be able cite an existing Consensus
Statement on everything which follows, which had been published in a
peer reviewed journal, and which was written and/or signed by a dozen or so of the
most experienced vitamin D researchers/clinicians.
However, it would be easier to herd cats than to organize these busy
people to work on such an article together. Until such an article is
written, an FLCCC Protocol along the following lines will help hundreds
of thousands of clinicians and researchers, and so millions of people.
Introduction
Since humans left African and other equatorial regions for higher
latitudes, with darker winters and shallower sun rays even in
mid-summer, inadequate circulating 25-hydroxyvitamin D has diminished
the health of an increasing proportion of the world's population.
Today, most people can only attain the 50 ng/mL (125 nmol/L) level of
circulating 25-hydroxyvitamin D which their immune systems need to
function properly by taking supplemental vitamin D3 in quantities -
which while small - are typically 8 or more times the very small
quantities recommended by governments and many doctors today.
This Protocol provides:
- Guidance on how much vitamin D3 to supplement, as ratios of body
weight, with higher ratios for those suffering from obesity. This
is required for the good health of almost all people, in all countries,
of all ages and body morphologies.
These recommendations are appropriate for people of all ages, from
newborns to the elderly, except when there is medical advice to the
contrary, concerns about hypercalcemia due to granulomatous disorders
or some cancers, and excepting infants substantially breast fed by
25-hydroxyvitamin D replete mothers.
- The best methods of 25-hydroxyvitamin D repletion in clinical emergencies such as sepsis and COVID-19: oral calcifediol (which is
25-hydroxyvitamin D) or a loading dose of vitamin D3. These
techniques take about 4 hours and 4 days, respectively, to boost the
level of circulating 25-hydroxyvitamin D safely over 50 ng/mL (125
nmol/L) from typical baseline levels between 5 and 20 ng/mL.
- A
tutorial introduction to the three "vitamin D" compounds and especially
their roles in little-known intracrine and paracrine signaling systems,
which the immune system and some other systems rely upon for each of
their cells to respond to their individual circumstances. This
includes correcting some common errors of terminology and
understanding, such as the oft-repeated statement that "vitamin D is a
hormone".
- Discussion
of the Coimbra and similar high 25-hydroxyvitamin D
protocols which suppress a wide range of chronic inflammatory
disorders, and the role of helminths and evolution in the current very
high prevalence of these disorders. The Coimbra and similar
protocols are a promising approach to treatment, but at
present the FLCCC does not have the expertise or experience to
recommend how they should be applied.
Compared to many aspects of biology and medicine, the function and
interactions of the three "vitamin D" compounds and their related
enzymes and receptor are not complex. Unfortunately, very few
clinicians, immunologists and even researchers understand the crucial
role 25-hydroxyvitamin D to calcitriol (1,25-dihydroxyvitamin D)
intracrine and paracrine signaling play in many types of immune cells,
and in cells of other types which are unrelated to immunity or
calcium-phosphate-bone metabolism.
This biology is relatively easy to understand. We are trying
to bring forward the day when professionals in medicine and other
related fields all clearly understand this biology, and so the need for
most people, of all ages, to supplement vitamin D3 properly. This
will constitute
a revolution in human health at least as significant as those which
have resulted
from sanitation, antibiotics, anesthesia and medical imaging.
Perhaps the greatest challenge in raising awareness of the importance
of proper vitamin D3 supplementation is overcoming the objection, which Prof.
Sunil Wimalawansa has frequently encountered in nearly three decades
of research and advocacy: "How could it be true? Its too
simple." In other words: "Isn't this just another
over-hyped nutritional supplement?".
How indeed could a simple nutritional supplement, available at every
supermarket and pharmacy, be the key to (very approximately) halving
the burden of human ill-health, as veteran vitamin D researcher Bill
Grant estimates?
One reason is that multinational pharmaceutical companies have many
billions of dollars in annual profits to lose if everyone's immune
systems ran properly from 50
ng/mL (125 nmol/L) circulating 25-hydroxyvitamin. Of all the
nutritional deficiencies, this is the most important and also the
easiest to prevent. (Boron, omega 3 fatty acids, magnesium and
especially potassium need to be taken either every day and/or involve
much greater quantities than vitamin D3 supplementation requires.)
Pharma grade vitamin D3 is made in only a handful of competitive
factories worldwide, none of them owned by multinational pharmaceutical
companies. The mainstream pharmaceutical industry has long waged
a campaign of dismissal, distraction and denial
against proper vitamin D3 supplementation. See Bill Grant's 2018
article Vitamin D acceptance delayed by Big Pharma following the Disinformation Playbook http://orthomolecular.org/resources/omns/v14n22.shtml. Other reasons include:
- Vitamin D research has traditionally been within the field of
endocrinology, since it initially centered on the well-understood hormonal
function of calcitriol by which the kidneys affect the function of
multiple cell types which are involved in calcium-phosphate-bone
metabolism.
- Only in the past two decades have researchers elucidated the role
of calcitriol as an intracrine and paracrine agent in three of the many
types of immune cell which rely on these signaling systems in order to
alter their behavior according to each cell's individual
circumstances.
- Absent an understanding of these systems, clinicians and
researchers have tended to assume that the mechanism by which "vitamin
D boosts the immune system" is by raising the stable and very low (ca.
0.07 ng/mL) level of circulating hormonal calcitriol. However
immune cells are not affected by this, and raised 25-hydroxyvitamin D
levels only marginally raise the hormonal calcitriol level.
The need for 50 ng/mL or more 25-hydroxyvitamin D
A section below discusses and cites some of growing body of research
which shows that the ability of the immune system to properly tackle
cancer and infections caused by bacteria, fungi, yeast and viruses
depends on it being supplied with 25-hydroxyvitamin D from the
bloodstream, at a level (concentration) of at least 50 ng/mL (125
nmol/L). It is reasonable to assume that this level, at least, is
also needed for the immune system to be able to properly tackle
multicellular parasites, and to reduce the risk of excessive
inflammatory (indiscriminate cell destroying) immune responses to other
types of infection, and in auto-immune responses to the body's own
healthy cells.
This Protocol is a step towards ensuring that all people have at least
this level of 25-hydroxyvitamin D, which is necessary for good
health. Since this level is central to all that follows, here we
briefly describe the research by doctors at Massachusetts General
Hospital which most clearly measures this need for 50 ng/mL circulating
25 hydroxyvitamin D. (#Quraishi-2014)
Over 9 years, the doctors performed Roux-en-Y gastric bypass operations
for weight loss on 770 severely obese patients. They recorded
their patients' circulating 25-hydroxyvitamin D level before the
operation and analyzed how this was associated with the risks of both
hospital acquired and surgical site infections after the
operation. The results were striking, and should have become
widely discussed and known to medical professionals, immunologists and
public health officials all around the world:
The patients whose pre-operative 25-hydroxyvitamin D was 50 ng/mL or
more would surely have attained this by substantial vitamin D3
supplementation. These patients had a very low, ca. 2.5%, risk of
both types of infection.
The risk for other patients rose significantly, and then drastically,
the further below 50 ng/mL their 25-hydroxyvitamin D level was before
the operation. 25-hydroxyvitamin D levels are fairly stable
week-to-week, and so are a good measure of the level during the
operation and in recovery. Here we observe a highly clinically
significant increase in infection, due to increasing degrees of immune
system failure, the further the 25-hydroxyvitamin D level was below 50
ng/mL.
Of all the research to date, this is the most direct, clear and
easy-to-understand measure of immune system dysfunction, regarding
responses to the primarily bacterial pathogens which cause these types
of infection, as a function of circulating 25-hydroxyvitamin D level.
The red curves are direct from the journal article's graphs. The
dotted area at the lower left approximately depicts the distribution of
25-hydroxyvitamin D levels among the general population, in most or
perhaps all countries, for people who are not supplementing vitamin D3
in quantities similar to those recommended by this Protocol. Some
people follow government vitamin D3 supplementation recommendations,
but these are for average daily amounts which are too small to
generally attain 50 ng/mL circulating 25-hydroxyvitamin D or more. The
primary aim of this protocol is to have everyone, of all ages, in all
countries, attain levels above 50 ng/mL, and generally no more than 100
ng/mL.
Vitamin D3 supplemental intake quantities
Vitamin D3 is superior to Vitamin D2
Vitamin D3 calciferous, which is produced in the skin by the action
of UV-B light on 7-dehydrocholesterol is the natural form of vitamin
D. Vitamin D2 ergocalciferol has a somewhat different molecular
structure and is typically made by irradiating a compound derived from
yeast. Vitamin D2 is inferior in all respects to vitamin D3, as
are its first and second hydroxylated versions 25-hydroxyvitamin D2 and
1,25-dihydroxyvitamin D2 to the natural D3 hydroxylates. (#Houghton-2006, #Jones-2014, #Nasim-2019, #Durrant-2022.)
Here we discuss vitamin D3 and its first and second hydroxylates, but
for brevity omit the '3': 25-hydroxyvitamin D calcifediol (also known
as calcidiol) and 1,25-dihydroxyvitamin D calcitriol.
Vitamin D2 should only be used if D3 is not available. Most
supplemental vitamin D3 is manufactured by irradiating
7-dehydrocholesterol, which is derived from wool fat. (#Hirsch-2010) For those seeking a vegan source of vitamin D, vitamin D3 extracted from algae is more effective than vitamin D2.
Food and ultraviolet B light
Food - including that which is fortified with vitamin D3 or the more
stable vitamin D2 ergocalciferol - can provide only a small fraction of
the vitamin D2/3 needed to maintain a healthy level of circulating (in
the bloodstream) 25-hydroxyvitamin D. This is made, primarily in
the liver, by hydroxylating vitamin D3 cholecalciferol at the 25th
carbon. The level (concentration) of 25-hydroxyvitamin D is
measured in "vitamin D" blood tests.
Ultraviolet B skin radiation can produce sufficient vitamin D3 to
maintain 50 ng/mL (125 nmol/L) or more circulating 25-hydroxyvitamin
D. However, this UV-B always damages DNA and so raises the risk
of cancer, so UV-B skin exposure is not a sustainable way to attain healthy
25-hydroxyvitamin D levels in the long-term. Furthermore,
pigmented skin greatly reduces the production of vitamin D3.
Clothing, housing and vehicular transport all greatly reduce the amount
of skin exposure to the UV-B component of sunshine, for good reason. Most people,
worldwide, live in locations where solar UV-B flux is too low for
substantial amounts of cutaneous vitamin D3 production, in white skin,
except in the middle of cloud-free mid-summer days.
So neither a "balanced diet" nor any practical, sustainable and safe
level of exposing the skin to sunshine or artificial UV-B light can
provide more than a fraction of the vitamin D3 we need to be healthy.
Many people think that any sunshine at all will enable their skin
to
produce significant amounts of vitamin D3, depending on its angle of
incidence at the skin and on the area of skin which is exposed.
However, this is only possible with high elevation sunlight.
Generally, if the Sun is closer than 45° from the horizon, the longer
path through the ozone layer and lower atmosphere significantly
attenuates the ca. 293 nanometer UV-B light which best generates
vitamin D3. This light is at the far high-frequency end of the
Sun's spectrum, and of what wavelengths can reach ground level through
the atmosphere.
People with brown or black skin cannot rely on sun exposure to generate
the full amount of vitamin D they need to be healthy, unless perhaps
they spend most of their days outdoors, within 20° of so of the
equator, with most of their body exposed and with no seasonal
interruption from the monsoon.
Mihauchi and Nakajima provide a detailed treatise on vitamin D3
production in the skin upon exposure to ultraviolet B light. (#Miyauchi-2016)
They advise that in order to maximize production, in any one day, no
further benefit is achieved by exposing the skin to more than 1/3 of
whatever amount of UV-B would be required to turn it somewhat red. They
advise that UV-B light, such as from sunlight, can produce the amount
of vitamin D3 needed for good health with relative safety.
However, the amount they assume is needed for adults is only 15
micrograms (600 IU) per day, which is about 1/8th of what we recommend
for 70 kg body weight. They estimate that 10 micrograms can be
produced by a UV-B exposure of 1/3 of what would redden the skin, over a
600 square cm area of skin. This is about 25 cm, or 10 inches,
square. Since average weight adults need about 50 times
this, every day, to be healthy, it follows from their estimates that
this would require the daily exposure of 3 square meters (32 square
feet) of skin, which is impossible
If supplements were not available, it would be healthy to get at least some
of the vitamin D3 we need via UV-B skin exposure, including by using
special UV-B lamps with which eye protection must be used.
Fortunately, supplemental vitamin D is readily available, and involves
no expenditure of time, or reliance on weather, location or the use of
special lamps.
Sunil
and Bill, do you recall an article which reported on lifeguards, at
beaches or pools in Hawaii, or perhaps California, who spent a lot of
time in the sun but only attained mean 25(OH)D levels in the mid-40
ng/mL range? I think people greatly overestimate their
ability to get sufficient vitamin D from being outdoors, even in summer.
Conventional recommendations and units
Government supplemental vitamin D3 guidelines are intended only to
attain the 20 ng/mL (50 nmol/L, 1 part in 50,000,000 by mass) level of
circulating 25-hydroxyvitamin D which the kidneys need to play their
role, with the parathyroid gland and osteocytes, in regulating
calcium-phosphate-bone metabolism. These very small recommended
vitamin D3 supplemental intake quantities, for adults, such as 15 to 20
mcg (the medical abbreviation for microgram) a day, on average,
probably achieve this goal in many adults, but will not do so for many
who are suffering from obesity.
Vitamin D3 daily supplemental quantities are commonly expressed in units of:
- International Units, also known as "IU"s or just "units". One IU of vitamin D3 = 0.025 micrograms = 1/40,000,000th of a gram.
- Micrograms, abbreviated to "mcg" or, in science "µg" (lower case Greek letter Mu) or "ug". One microgram = 40 IU.
- More rarely, as milligrams "mg". One milligram = 1/000th gram = 40,000 IU.
Government guidelines, which are followed by most doctors worldwide,
specify supposedly adequate amounts of vitamin D3 per day as fixed
amounts for whole groups of people, stratified by age, with little or
no account for body weight. (#Kimball-2020).
Recommended Daily Allowance (RDA)
The RDA is the amount of a nutrient to be ingested, per day, so that
97.5% of the target population have enough of this nutrient, or
whatever the body converts it to, in order to be healthy. In the
United States and Canada - and more broadly in many countries - the
most influential determination of an RDA for vitamin D3 was made in
2011 by the IOM (Institute of Medicine) (#IOM-2011). For adults this is 15 micrograms = 600 IU per day, on average.
RDAs are intended to be directly used as guidelines for
supplementation, after considering how much of the nutrient is
typically consumed in food.
This Protocol cites numerous research articles which establish, beyond
doubt, that for 70 kg 154 lb body weight, without obesity, it is
necessary to gain (via food, supplements or cutaneous production),
about 125 micrograms (5000 IU) vitamin D3 a day, on average, in order
to attain at least the 50 ng/mL (125 nmol/L = 1 part in 20,000,000 by
mass) level of circulating 25-hydroxyvitamin D which the immune system
needs to function properly.
This is an 8 times the IOM's RDA. Even if the IOM's 20
ng/mL (50 nmol/L) 25-hydroxyvitamin D target level is assumed to be
valid, the IOM's RDA is far too low, due to faulty statistical
calculations, as was pointed out in detailed critiques. (#Veugelers-2014, #Heaney-2015)
However, the IOM's vitamin D3 recommendations have never been revised.
They form the basis of many governments' official recommendations to
this day.
There are numerous problems with RDAs, especially in the case of vitamin D3:
- For any given target population, the RDA is set almost
entirely by how much vitamin D3 per day is required for the people in
the 97.5%
body weight percentile of the population to attain the desired
25-hydroxyvitamin D level. (Individual variation in absorption
and hydroxylation efficiency is the other factor.)
In practical terms, this can be estimated only very approximately due
to the difficulties in sampling individuals to participate in a
clinical trial, lasting six months or more, with different intake
quantities, since it takes this long for 25-hydroxyvitamin D levels to
stabilize. The expense of such trials for individual countries is
prohibitive.
- Mens' body weight, on average, exceeds that of women's.
- For any given country or ethnicity, individual body weights vary
widely for any class of person, such as "1 - 18 years" or "18 to 70
years", which are two of the classifications found in government
vitamin D3 supplemental intake recommendations. (#Kimball-2020).
- Average body weights vary widely between countries /
ethnicities. Extremes of the distribution are represented by
Bangladesh and Tonga, with M / F mean body weights 55.2 / 49.8 kg in
Bangladesh and 98.6 / 95.5 kg in Tonga. (#WHO-2010, #WHO-2012)
- For any given amount of vitamin D3 supplemental intake, as a
ratio of body weight, the level of 25-hydroxyvitamin D which is
attained in the long term is lower in those suffering from obesity, for
at least two reasons: Lower rates of hydroxylation, primarily in the
liver; and Increased sequestration of 25-hydroxyvitamin D and/or
vitamin D3 in the excess adipose tissue. (#Roizen-2019, #Elkhwanky-2020, #Zhu-2021)
Obesity and ratios of body weight
Since good health can only be attained with 50 ng/mL (125 nmol/L) or
more circulating 25-hydroxyvitamin D and since this can, with rare
exception, only be safely and practically achieved by ingesting an
appropriate average daily quantity of supplemental vitamin D3, for our
entire population to attain good health it is necessary for most
individuals to supplement a well chosen quantity of vitamin D3, on
average per day.
Even in wealthy nations, it would be impractical and a waste of
precious resources to ensure proper 25-hydroxyvitamin D levels through
iterations of changes to supplemental vitamin D3 intake quantities,
under the guidance of healthcare professionals, with typically multiple
25-hydroxyvitamin D blood tests.
Such medical attention and the requisite test facilities are not available in developing countries.
It is both necessary, and broadly sufficient, to choose the
supplemental vitamin D3 intake quantity as a ratio of body weight, with
higher ratios for those suffering from obesity.
Fortunately, a wide range of intake quantities, for any individual is
broadly healthy. Many medical professionals today are not
aware that at least 50 ng/mL (125 nmol/L) circulating 25-hydroxyvitamin
D is required for full immune system function. Furthermore, the
lower, average, levels of whole populations and an overly alarmist,
poorly informed, understanding of toxicity mechanisms leads many
medical professionals to regard levels which are in fact perfectly
healthy - such as 50 to 100 ng/mL (125 to 250 nmol/L) - as dangerously
high. A section below reviews the toxicity concerns which arise
with higher 25-hydroxyvitamin A levels than this, which generally begin above 150 ng/mL.
Self regulation of 25-hydroxyvitamin D level
Some nutrients, such as iron, are difficult to substantially supplement
because humans have no proper mechanism for lowering the accumulated
level. The body is tolerant of a large range of vitamin D3
supplemental intake quantities in part because there is a broad,
self-limiting, system by which higher circulating 25-hydroxyvitamin D
levels lead to greater activity of a 24-hydroxylase enzyme. This
irreversibly hydroxylates vitamin D3, calcitriol and most importantly,
circulating 25-hydroxyvitamin D, on the 24 carbon, which renders the
molecule inactive and destined for breakdown.
Sunil
and Bill, can you suggest one or two good references for this
self-limiting process? It is generally regarded as being
controlled by calcitriol levels. This might be true in lab
experiments, but increased circulating 25(OH)D levels only marginally
boost circulating calcitriol levels. Where are these enzymes
located? I recall reading that the activity of these enzymes was
significantly - largely? - controlled directly by circulating 25(OH)D
levels, which makes sense, since this is
what needs to be controlled. I guess this happens simply because
25(OH)D has a small, but significant, affinity for VDR, and that VDR
activation somehow controls the activity of the enzyme wherever it
matters most for reducing circulating levels. There's no
need to explain it in such detail here, but it would be great to have
one or two pertinent references.
The effect of this self-regulating mechanism can be seen in the curved
lines of a graph which plots long-term circulating 25-hydroxyvitamin D
levels against daily average vitamin D3 intake quantities, for
underweight, normal weight, overweight and obese adult subjects, in
Ekwaru et al.'s The Importance of
Body Weight for the Dose Response Relationship of Oral Vitamin D
Supplementation and Serum 25-Hydroxyvitamin D in Healthy Volunteers. (#Ekwaru-2014)
I
will make an updated, simpler, version of this graph. The
original Fig 3 is poorly labeled and only shows the 25(OH)D level in
nmol/L and the intake quantities in IUs. I will make the green
area extend from 50 ng/mL to the top of the graph.
Vitamin D3 supplemental intake quantities as three ranges of ratio of body weight
The term "dose" is used in medical interventions. Here we are
discussing long-term nutrition, so we use "supplemental intake
quantity".
The introductory material above is sufficient to support an
appreciation of the need for vitamin D3 supplemental intake quantity
recommendations which are generally applicable to all people in the
absence of medical advise to the contrary, as ratios of body
weight, with higher ratios for those suffering from obesity.
Sections below cite research which establishes the need for at least 50
ng/mL (125 nmol/L) circulating 25-hydroxyvitamin D and a tutorial
explanation of the 25-hydroxyvitamin D to calcitriol intracrine and
paracrine signaling systems which many types of immune cell rely upon,
and which to the best of our knowledge can only operate properly with
at least this level of circulating 25-hydroxyvitamin D.
These recommendations are Prof Sunil Wimalawansa's simplification and
revision of his earlier work - the first such recommendations in the
peer-reviewed literature - which were incorporated into some FLCCC
Protocols in 2022. (#Wimalawansa-2022)
Each recommendation is a range of ratios, by which a body weight can be
multiplied to give lower and upper amounts of vitamin D3, on average,
per day, to supplement. The exact amount to supplement is not
critical. It is more important to choose an amount which can be
conveniently supplemented, such as by a single 1.25 milligram 50,000 IU
capsule once a week, or once every ten days.
The half-life of circulating 25-hydroxyvitamin D is long enough at 50
ng/mL that larger quantities every week to ten days will not lead to
significant variations in level. Gaps of longer than this
between vitamin D3 intakes should be avoided.
The ranges of ratios do not overlap. This does not mean that
an individual who at one point in time is overweight, and later becomes
obese - even though the increase in body weight is only marginal, such
as 10% - should suddenly switch from the first set of ratios to
the second. If there is uncertainty about whether an individual
would be properly diagnosed as overweight, or obese, please use a range
of ratios between the two sets described below, such as 80 to 100 IUs
per kilogram body weight per day.
These recommendations have not been tested in a randomized controlled
trial (RCT). To do so would be a massive project which ideally
will be undertaken in the years to come.
The base range of ratios, for people with underweight, normal and
overweight body morphologies is derived from long-term observations of
Iranian doctors working in Dubai. (#Afshar-2020) In ten years of advising over 500 of their opthalmology patients, of all body morphologies, to supplement 70 to 100 IU vitamin D3 per kg body weight, per day, their observations included:
- Baseline (before the supplementation) 25-hydroxyvitamin D levels
of 95% of the patients was below 35 ng/mL (87.5 nmol/L). This is
in sunny Dubai, 25° from the equator, similar to Miami, Hyderabad,
Taipei, Southern Brazil, Johannesburg and central Queensland.
- All patients attained, over several years, between 40 ng/mL and
90 ng/mL (100 to 225 nmol/L) circulating 25-hydroxyvitamin D.
There was no toxicity.
This outcome - all 500+ patients within +/- 38% of 65 ng/mL is a much
narrower and healthier distribution than would resulted from all these
adults, with their differing body weights and obesity states, taking any single, exactly defined, quantity of vitamin D3 per
day, on average.
In this distribution of circulating 25-hydroxyvitamin D levels, those
with the lowest levels would have been
those who were suffering from obesity. A pure body weight ratio
is fine for people who have the same general proportion ingested
vitamin D3 converted to circulating 25-hydroxyvitamin D. For most
people who are not suffering from obesity, this proportion is, very
approximately, 1/4. However, the proportion is lower for those
suffering from obesity.
For everyone's level to be safely over 50 ng/mL, without raising the level
of those at the higher end of the distribution, it suffices to choose a
greater ratio of body weight for those suffering from obesity, to
compensate for their less efficient conversion of vitamin D3 to
25-hydroxyvitamin D.
The two other ranges of ratios presented below, for those suffering
from obesity I and II and for those suffering from obesity III, are the
result of Professor Wimalawansa's judgments according to clinical
experience, great familiarity with the research in general, and in
particular the observations and suggestions found in (#Ekwaru-2014)
and in the 2011 Endocrine Society Clinical Practice Guidelines, which
aimed to attain at least 30 ng/mL (75 nmol/L) circulating
25-hydroxyvitamin D. (#Holick-2011)
Sufficient vitamin D3 from breast feeding or UV cutaneous production
There is no need for substantially breast-fed infants to be given
supplemental vitamin D3 as long as their moms have good
25-hydroxyvitamin D levels: 50 ng/mL (125 nmol/L) or more.
People with light or moderately pigmented skin who in recent months
have received sufficient UV-B skin exposure to tan significant areas of
their body need less supplemental vitamin D3, and some may need none in
order to attain at least the desired 50 ng/mL level of circulating
25-hydroxyvitamin D. Few people can do this all year round.
While outdoor living and sun exposure in general have many health
benefits, people who generate sufficient vitamin D3 in their skin,
for extended periods of time, to attain this desired level, would
probably improve their health by protecting their skin from ultraviolet
light to a greater extent, and taking some fraction of the supplemental
vitamin D3 quantities recommended in the following subsections.
Adverse reactions and potential toxicity
By the standards of the IOM and those adopted by most government
regulatory agencies, which ignore the role of 25-hydroxyvitamin D in
the immune system, 50 ng/mL is a relatively high level and 100 ng/mL is
very high indeed. However, in the only research which measured
25-hydroxyvitamin D in people assumed to be living like our African
ancestors, the mean level of traditionally living East African Maasai
herders and Hadzabe hunter gatherers, mean age 34, was 46 ng/mL (115
nmol/L). (#Luxwolda-2012)
Conventional vitamin D toxicity - 25-hydroxyvitamin D levels above 150
ng/mL (375 nmol/L) which for some people may cause hypercalcemia
(excessive calcium ion levels in the bloodstream) and/or loss of calcium
in the bone - will not occur when the recommendations below are followed.
We regard 100 ng/mL (250 nmol/L) as the high end of the normal, healthy
range, but there is no need for alarm if the level exceeds this
modestly. From the 2011 Endocrine Society Guidelines:
Although it is not known what the safe
upper value for 25(OH)D is for avoiding hypercalcemia, most studies in
children and adults have suggested that the blood levels need to be
above 150 ng/mL before there is any concern. Therefore, an upper limit of 100
ng/ml provides a safety margin in reducing risk of hypercalcemia.
The clinicians and researchers who wrote these guidelines, and who have
been proven to be wiser than those who wrote the IOM guidelines, were
not concerned about 150 ng/mL circulating 25-hydroxyvitamin D. They applied a large, arbitrary,
33% safety margin to arrive at 100 ng/mL So there is no need to
apply further margins and so become concerned with levels such as, for
instance, 90 ng/mL or 100 ng/mL, or even, in the great majority of cases, 140 ng/mL.
While this excessive 25-hydroxyvitamin D level tends to raise
circulating calcitriol levels, when disregulation of calcium ion
levels, leading to hypercalcemia occurs, this is not necessarily due to
the somewhat elevated calcitriol level. Hypervitaminosis D
(excessive, for that individual, circulating 25-hydroxyvitamin D)
causes hypercalcemia largely or entirely due to the larger number of 25-hydroxyvitamin D
molecules binding to VDR (the "vitamin D" - really the calcitriol -
receptor) molecules, to which they have a small, but in these
circumstances significant, affinity. (#Tebben-2015)
Hypercalcemia can also occur without excessive 25-hydroxyvitamin D levels, such as due to genetic variations, an isomer of
25-hydroxyvitamin D which has higher affinity for VDR and malfunction of the
24-hydroxylase enzyme which degrades calcitriol and the other two
compounds. (#Tebben-2015)
Conventional treatments for these conditions for patients whose
25-hydroxyvitamin D levels are typically well below 50 ng/mL may not be
appropriate for those with levels between 50 and 100 ng/mL, which are
the limits of the levels likely to be attained by following the
recommendations below. Suspected or confirmed hypercalcemia should
be regarded as contraindicating vitamin D3 supplementation unless there
well informed medical advice that it is safe to do so.
Insight into the long-term safety of substantial vitamin D3
supplementation, in some cases with greater amounts than recommended
below, can be found in McCullough et al. 2019, who reviewed long-term
vitamin D3 supplementation of adult patients in a psychiatric hospital
with 125 or 250 micrograms (5000 or 10,000 IUs) of vitamin D3 a day. (#McCullough-2019) Since 2011:
. . . we have admitted over 4700
patients, the vast majority of whom agreed to supplementation with
either 5000 or 10,000 IU/day. Due to disease concerns, a few
agreed to larger amounts, ranging from 20,000 to 50,000 IUs/day.
There have been no cases of vitamin D3 induced hypercalcemia or any
adverse events attributable to vitamin D3 supplementation in any
patient. Three patients with psoriasis showed marked clinical
improvement in their skin using 20,000 to 50,000 IUs/day.
The mean 25-hydroxyvitamin D level of patients not supplementing
vitamin D3, and of the baseline levels of those who did, was 27 ng/mL
(68 nmol/L). The researchers report no sign of hypercalcemia in the patients who supplemented vitamin D3:
Analysis of 418 inpatients on D3 long
enough to develop 25(OH)D blood levels > 74.4 ng/mL showed a mean
25(OH)D level of 118.9 ng/mL, with a range from 74.4 to 384.8
ng/mL. The average serum calcium level in these 2 groups was 9.5
(no D3) vs. 9.6 (D3), with ranges of 8.4 to 10.7 (no D3) vs. 8.6 to
10.7 mg/dl (D3), after excluding patients with other causes of
hypercalcemia.
The great majority of the population, of all ages, who adopt vitamin D3
supplementation to attain at least 50 ng/mL (125 nmol/L circulating
25-hydroxyvitamin D will derive profound health benefits with respect
to their prior condition of much lower levels, which had reduced, including
to the point of crippling, their immune system's ability to respond to
cancer cells and bacterial, fungal, viral and multicellular parasitic
pathogens.
However, among large numbers of people adopting this generally very
healthy supplementation arrangement, there may be a few who suffer
adverse reactions which have not yet been adequately observed and
reported in the peer-reviewed literature. If any adverse reaction
to vitamin D3 supplementation is suspected, the supplements should be
stopped immediately and medical advice
sought. See #Appendix-1 for notes on
some indications that vitamin D3 supplementation may, for some
individuals precipitate heart arrhythmias, despite such supplementation,
in the general population, reducing the incidence of a major form of
such arrhythmias: atrial fibrillation.
One class of conditions in which vitamin D3 supplementation is
conventionally considered undesirable is granulomatous disorders such
as sarcoidosis. The immune system fails to regulate itself
properly (likely due, in part, to inadequate circulating
25-hydroxyvitamin D) and multiple types of immune cell cluster together
in a disordered, self-destructive, excessively inflammatory,
response. It as if the immune cells are fighting among
themselves, for no good purpose. Macrophages, in a spurious and
undesirable activation of their intracrine/paracrine signaling systems,
continually hydroxylate 25-hydroxyvitamin D to calcitriol. This
can occur to such a degree, in the whole body, that the calcitriol
which diffuses from these cells significantly raises the very low level
of circulating, hormonal, calcitriol, above the level which the kidneys,
on their own, would maintain in order to achieve optimal calcium
levels. The result is potentially harmful or life-threatening
hypercalcemia. However, Kamphius et al. report that sarcoidosis
patients do better with supplemental vitamin D3 and calcium. (#Kamphius-2014)
The Cancer Monograph currently does not mention hypercalcemia of malignancy.
This is a serious omission since this is apparently a problem in up to
20% of cancers, and may conventionally regarded as a reason not to raise
25-hydroxyvitamin D levels, especially as high as this Protocol intends.
Hopefully Dr Dalgleish can advise on this.
A second class of such conditions is a subset of cancers in which
large
numbers of tumor-adjacent macrophages continually hydroxylate
25-hydroxyvitamin D to calcitriol. This can
lead to hypercalcemia secondary to elevated circulating (hormonal)
calcitriol levels. This sustained activity would surely deplete
25-hydroxyvitamin D in the vicinity of the tumor, which would reduce
the immune system's ability to eliminate the
aberrant cells. These cancers include some types of
lymphoma. (#Hewison-2009)
Long-term 50 ng/mL or more circulating 25-hydroxyvitamin D will reduce
the risk of cancers developing and spreading. While this and
emergency 25-hydroxyvitamin D repletion to this or higher levels will
generally greatly strengthen immune responses to malignant cells, FLCCC
protocols do not currently include recommendations on how best to
tackle hypercalcemia of malignancy.
Several types of cancer involve risk of hypercalcemia. Those with
suspected or diagnosed cancer should seek specialist medical attention,
especially concerning the risk of hypercalcemia and to what extent this
would contraindicate vitamin D3 supplementation. (#Sternlicht-2015, #Tebben-2015)
Authoritative guidance in Treatment of Hypercalcemia of Malignancy in Adults: An Endocrine Society Clinical Practice Guideline includes a variety of treatments. (#Fuleihan-2023)
The authors do not specifically advise against cessation of vitamin D3
supplementation. However, most of their patients would have
supplemented little or no vitamin D3. They state:
To avoid hypocalcemia in adults with
HCM who receive antiresorptive therapy, vitamin D levels should be
monitored and managed in accordance with Endocrine Society vitamin D
guidelines.
However, these guidelines are intended to attain ca. 20 to 30 ng/mL (50
to 75 nmol/L) circulating 25-hydroxyvitamin D, while the
recommendations below will attain two to three times this.
6 months or so for 25-hydroxyvitamin D levels to stabilize
Sunil
and Bill: Is this a reasonable description? To what extent is
25(OH)D stored in the liver? The livers of at least some other
vertebrates contain significant amounts of vitamin D3 and/or 25(OH)D.
Ingested vitamin D3 is hydroxylated, primarily in the liver, over a
period of a week or so, to circulating 25-hydroxyvitamin D. The
level of circulating 25-hydroxyvitamin D takes months to to stabilize
close to its long-term value, in part due to this level being coupled
to 25-hydroxyvitamin D absorbed in adipose and other tissues, and which
is to some extent later available to diffuse back into circulation.
This is clearly visible in time-series graphs of adults taking 125 and
250 micrograms (5000 and 10,000 IU) vitamin D3 a day in an Ohio
psychiatric hospital. (#McCullough-2019)

Higher initial supplemental intake to boost 25-hydroxyvitamin D level more rapidly
Anyone who has not been supplementing vitamin D properly, as described
below, or has been doing so for a month or two, and is facing a
clinical emergency, such as:
- Sepsis;
- COVID-19, influenza, ARDS or any other infectious disease in
which there is already, or in which there is significant risk of,
serious symptons; or
- Cancer;
- Recovery from surgery, severe injury or extensive burns;
should consult the next section on using calcifediol or a loading dose
of vitamin D3 to boost 25-hydroxyvitamin D levels as rapidly as
possible.
Pregnancy arguably presents an urgent need for attaining at least 50
ng/mL circulating 25-hydroxyvitamin D, for reasons discussed in a later
section. Since the fetus' brain is building itself, and to reduce
the risk of perinatal complications, at all stages of pregnancy, the
impetus for 25-hydroxyvitamin D repletion is at its highest, since the
mother is at risk and the entire life of the future child hangs in the
balance.
Women of childbearing age are the group who most need to be
supplementing vitamin D3 properly. Since most of them don't, the
chance of pregnancy and any stage in pregnancy and afterwards is a
really good time to boost their 25-hydroxyvitamin D. The graphs
above show the slow rise of circulating 25-hydroxyvitamin D over months which results from proper
vitamin D3 supplementation, but this is too slow at any stage of pregnancy considering what is at stake.
Here we suggest how this might be done, for adults, including pregnant
women. Similar principles apply to infants and children.
The first step is to estimate the likely 25-hydroxyvitamin D of the
person, since 25-hydroxyvitamin D blood tests typically take days to
generate results, and may not be available. If the person is
known, or reasonably assumed, to have been supplementing little or no
vitamin D3 in recent months, and has not, in that time, had extensive
UV-B exposure of ideally white skin, then they can be assumed to have
25-hydroxyvitamin D levels no higher than 20 ng/mL (50 nmol/L).
The elderly and people with brown or black skin can be assumed to have
lower levels still, often down to 10 ng/mL (25 nmol/L). Even in
Israel, due to sun-avoidant clothing and lifestyle restrictions,
approximately 23% of Arab women had 10 ng/mL or less 25-hydroxyvitamin
D. 6% of these Arab women had 5 ng/mL or less, which is disastrously low. (#Israel-2020)
In the UK, 95% of people of Pakistani ethnicity were found to have 20
ng/mL or less 25-hydroxyvitamin D, averaging over all seasons.
65% had 10 ng/mL or less and 26% had 6 ng/mL (15 nmol/L) or less.
(#Darling-2020)
The following graph, prepared from UK Biobank data, depicts the
proportions of different ethnicities whose circulating
25-hydroxyvitamin D levels are below 30, 20 and 10 ng/mL, with seasonal
variation. (#Sutherland-2020 Table 2, the '%' signs are spurious.)

People who are known, or reasonably assumed, to have 25-hydroxyvitamin
D levels of 15 ng/mL (37.5 nmol/L) or less can accelerate the
rate at which their levels rise to much safer values, such as 40 ng/mL
125 nmol/L by, for instance:
- Doubling their supplemental intake for the first 8 weeks.
- Quadrupling it for the 4 weeks.
- Multiplying the amount by 8 for the first 2 weeks.
These approaches bring 8, 12 and 14 weeks, respectively worth of
vitamin D3 forward, into shorter periods.
Those with
25-hydroxyvitamin D levels likely to be in the 15 to 30 ng/mL (37.5 to
75 nmol/L) range may wish to accellerate the rise in their levels as
shown above, but for 4, 2 and 1 week respectively.
For underweight, normal weight and overweight people
Subject to the above-mentioned exclusions (medical advise to the
contrary, any apparent adverse reactions, conditions which may cause
hypercalcemia and infants substantially breast-fed by 25-hydroxyvitamin
D replete mothers), we recommend that all people, of all ages, except
those suffering from obesity, supplement vitamin D3 with daily
average quantities within the following ranges of ratios of body weight.
70 to 90 IU per kilogram
32 to 41 IU per pound
1.8 to 2.3 micrograms per kilogram
0.8 to 1.0 micrograms per pound
For particular body weights in kilograms, the following
table shows the pounds equivalent and the recommended range of average
daily vitamin D intake quantities in IUs and micrograms.
Kilograms
|
Pounds
|
IUs/day
|
Micrograms/day
|
5
|
11
|
350 - 450
|
9 - 11
|
10
|
22
|
700 - 900
|
18 - 23
|
15
|
33
|
1050 - 1350
|
26 - 34
|
20
|
44
|
1400 - 1800
|
35 - 45
|
30
|
66
|
2100 - 2700
|
53 - 68
|
40
|
88
|
2800 - 3600
|
70 - 90
|
50
|
110
|
3500 - 4500
|
88 - 113
|
60
|
132
|
4200 - 5400
|
105 - 135
|
70
|
154
|
4900 - 6300
|
123 - 158
|
80
|
176
|
5600 - 7200
|
140 - 180
|
90
|
198
|
6300 - 8100
|
158 - 203
|
100
|
220
|
7000 - 9000
|
175 - 225
|
It is more important to find a convenient, easy to remember
arrangement for supplementation than to choose an average daily intake
of vitamin D3 which fits exactly within the recommended range. A
single daily capsule or
tablet, in addition to the small amount of vitamin D3 found in a daily
multivitamin capsule may be a good choice.
For instance, for 70 kg (154 lb) the recommended range of quantities is 4900 to
6300 IUs per day, on average. 5000 IU (125 micrograms) a day is a
perfectly good choice, which can be attained with a daily 5000 IU
capsule.
In countries such as Australia, where the largest capacity vitamin D
capsule or tablet which can be sold without prescription is 1000 IU (25
micrograms), it would be expensive, inconvenient and involve ingesting
potentially excessive carrier oil to consume five of these a day.
This is especially so in another example - 105 kg (231 lb) with obesity
1, as mentioned in the next section, for which a range between 10,500
and 13,650 IUs per day is recommended.
Sunil
and Bill: Can you suggest one or a few K2 references?
Should we add a section on vitamin K2, since it is widely available in
combination capsules with vitamin D3, and is a highly regarded
supplement? There are many commenters on Internet forums
who will chime in about the need or at least desirability of vit K2
supplementation as soon as anyone mentions vitamin D3 alone.
Better choices may involve a daily capsule with 100 micrograms or more
of vitamin K2 (which is generally beneficial for the immune system and
help retain calcium in the bone and reduce the risk of hypercalcemia)
and a small amount of vitamin D3, such as 1000 IU, with the difference
being made up with 50,000 IU capsules every 5, 7 or 10
days. In practice, 5000, 10,000 and 50,000 IU vitamin D3
capsules are available worldwide, including in Australia, via eBay and
Amazon, including from eBay sellers in Australia who may not be aware
of the regulations.
For instance the 105 kg person could take one of the many types of 5000
IU (125 microgram) vitamin D capsule which also contain vitamin K2, each day and take a
50,000 IU capsule once every ten days. With 200 IU vitamin D3 in
a daily multivitamin capsule, this would be 10,200 IU a day, on
average. With a weekly 50,000 IU capsule, this would be 12,343
IUs a day, on average.
Infants and young children should be given vitamin D3 drops.
We recommend choosing a well established brand of supplement, ideally made
in a developed country, since there are a plethora of supplement brands with no substantial history
available via online sellers, with low prices and a higher risk of not
meeting proper quality standards.
For children, adolescents and adults suffering from obesity I and II
These two stages of obesity are most simply defined as BMI in the range 30 to 39.
100 to 130 IU per kilogram
46 to 59 IU per pound
2.5 to 3.3 micrograms per kilogram
1.1 to 1.5 micrograms per pound
Body Mass Index is calculated by dividing the body weight, in
kilograms
by the square of the height, in meters. Alternatively, the
weight in pounds can be multiplied by 703 and then divided by the
square of the height in inches. For example, with 227 pounds and
71 inches, BMI = (227 * 703) / (71 * 71) = 31.7.
The BMI formula is most applicable to average height Caucasian
adults. It overestimates obesity for tall adults and
those with well developed musculature and underestimates it for short adults.
Obesity in childhood and early adolescence is best determined by
clinical diagnosis. Obesity in Asian adults may be
better determined by clinicians than by the BMI formula.
Kilograms
|
Pounds
|
IUs/day
|
Micrograms/day
|
40
|
88
|
4000 - 5200
|
100 - 130
|
50
|
110
|
5000 - 6500
|
125 - 163
|
60
|
132
|
6000 - 7800
|
150 - 195
|
70
|
154
|
7000 - 9100
|
175 - 228
|
80
|
176
|
8000 - 10,400
|
200 - 260
|
90
|
198
|
9000 - 11,700
|
225 - 293
|
100
|
220
|
10,000 - 13,000
|
250 - 325
|
120
|
264
|
12,000 - 15,600
|
300 - 390
|
140
|
309
|
14,000 - 18,200
|
350 - 455
|
For adolescents and adults suffering from obesity III
This is a serious, in-part inflammatory, metabolic disorder which
requires concerted medical attention. A BMI of 40 or more
indicates obesity III, but please see the notes above on the
superiority of clinical examination in making this diagnosis.
The recommended vitamin D3 supplemental intake quantity for those suffering from obesity III is expressed in four ways:
140 to 180 IU per kilogram
64 to 82 IU per pound
3.5 to 4.5 micrograms per kilogram
1.6 to 2.0 micrograms per pound
Kilograms
|
Pounds
|
IUs/day
|
Micrograms/day
|
80
|
176
|
11,200 - 14,400
|
280 - 360
|
100
|
220
|
14,000 - 18,000
|
350 - 450
|
120
|
264
|
16,800 - 21,600
|
420 - 540
|
150
|
331
|
21,000 - 27,000
|
525 - 675
|
190
|
419
|
26,600 - 34,200
|
665 - 855
|
240
|
529
|
33,600 - 43,200
|
840 - 1080
|
This is where I am up to.
Below are some rough headings to give an idea of the sections I am yet to complete.
Following those are the references and Appendix 1.
Rapid boosting of 25-hydroxyvitamin D to 50 ng/mL or more in clinical emergencies
Single oral dose of 0.014 mg calcifediol per kg body weight
(This is exactly as Prof. Wimalawansa recommends and has been incorporated into some FLCCC protocols.)
Sources of calcifediol
(There are Spanish capsules with 0.266 mg. Otherwise, it is hard
to obtain in substantial quantities. There are small 0.01
mg tablets available without prescription in the USA. 100 of
these provide 1 mg. This can be inconvenient. However, they
can be made into a drinkable, only slowly settling, slurry by adding a
little xanthan gum and mixing quickly with a small amount of cold
water. See, broadly: https://vitamindstopscovid.info/04-calcifediol/.)
Research supporting this calcifediol protocol
(The Faes Farma patent graph. Also, there was a similar graph
published in a journal, but very rarely cited, which showed the rapid
rise in 25(OH)D from oral calcifediol. I recall this was in
ca. 1976! Imagine how
many tens or hundreds of millions of lives would have been saved since
then if this discovery was linked to the immune system and made very
widely known.
Castillo et al. Some mention of the other Spanish research
trials, which did not have proper control groups and which took place
later, after many people in the area had started taking calcifediol at
home.)
Loading dose of vitamin D3
(I will find a simpler way of specifying the amount to use.
There is some research to cite on its effectiveness in the ICU in general, and with COVID-19.)
Tutorial on the three vitamin D compounds and on intracrine and paracrine signaling
(This will be a much more streamlined version of material at: https://vitamindstopscovid.info/02-intracrine/ and https://vitamindstopscovid.info/00-evi/#02-compounds.)
Vitamin D3 cholecalciferol
25-hydroxyvitamin D, calcifediol, 25(OH)D
1,25-dihydroxyvitamin D calcitriol
Intracrine signaling
(Sometimes, incorrectly, referred to as "autocrine" signaling, as I did initially, and did Chauss et al.)
Paracrine signaling
(The intracellularly produced calcitriol, made only in response to that
cell detecting a particular condition, diffuses to nearby cells,
presumably of different types, at a local level significantly higher
than the very low ~~0.07 ng/mL hormonal background level, and affects
the behavior of those other cells.)
The dependence on the immune system and other systems, such as
those concerning neurodevelopment and neuroprotection, on higher levels
of 25-hydroxyvitamin D than are commonplace today
(There's a vast amount of research which we can cite here, including
especially concerning COVID-19. The trick will be to select the
best and present it in a constructive way, better than the usual long
laundry list of vitamin D this, vitamin D that, citations in research
articles.
The 2008 Grassroots campaign for recognizing 40 to 60 ng/mL, recently
revived to tackle the terrible, recent, Endocrine Society Guidelines.
Many researchers and clinicians are endorsing this. Sunil has a
chart there which would be good to include in this FLCCC Vitamin D3
Supplementation Protocol:
Grassroots Health have some great charts showing disease severity vs. 25(OH)D, one of which is below.
There are various graphs of COVID-19 severity and 25(OH)D level I can adapt, including:

It would be best if I made a new diagram with 25(OH)D level on the horizontal axis, to match other diagrams.
The above diagram has a histogram I made from the raw Luxwolda et al.
2014 on Maasai and Hadzabe 25(OH)D levels. I have never seen this
data as a histogram.
The above diagram contains a copy of the histograms from Israel et al., which are most instructive:

I can redo all these graphics to better suit the FLCCC Protocol. See more diagrams of potential interest at:
By the time the reader gets to this section, they will have a very
clear idea of the mechanisms which underly this, which are all to do
with 25(OH)D >>> calcitriol intracrine and paracrine
signaling, and which have nothing to do with endocrinology, hormonal
signaling, or the level of circulating calcitriol.)
Inflammation, helminths and the Coimbra high 25-hydroxyvitamin D protocol
(Excessive, self-destructive, indiscriminate cell destroying
inflammatory immune responses cause a vast array of auto-immune
disorders, as well as being the central problem in sepsis.
The evolutionary reasons for this are understood by helminth
researchers, but vitamin D researchers and clinicians seem to know
little about it.
I think the helminth researchers and those who introduce helminths
infections to suppress auto-immune disorders never think about vitamin
D!
I think this FLCCC protocol should recognize the importance of these
mechanisms and suggest that the Coimbra and similar protocols be
considered. However, the FLCCC currently lacks the expertise and
experience to suggest exactly how to do it.
This is a fascinating and important field. I don't know of
any researchers or clinicians who discuss all this material together,
but they are clearly linked, since both helminthic therapy and the
Coimbra protocol successful suppress much the same set of disorders, by
completely different mechanisms, and these disorders are conventionally
regarded as incurable, or at least only suppressible by a dangerous mix
of drugs which suppress not just inflammatory immune responses but most
or all other immune responses.
I propose a much streamlined account of the research covered here:
Here is a brief account of these topics I wrote in a Substack comment recently.)
Helminthic therapy - introducing a helminth (intestinal worm) infestation - https:// helminthictherapywiki.org,
without any attention to typically very low 25-hydroxyvitamin D levels,
suppresses much the same set of diseases as the Coimbra and similar
protocols which raise 25-hydroxyvitamin D levels typically well above
100 ng/mL (250 nmol/L), without helminth infections.
See all the material at: https:// vitamindstopscovid.info/06-adv/
Helminthic therapy plus 50 ng/mL (125 nmol/L) 25-hydroxyvitamin D would
surely be better than just introducing helminths to people with
typically very low (compared to this level) 25-hydroxyvitamin D.
In 2022 I counted the testimonials at this German site run by doctors who use the Coimbra protocol: https:// www.coimbraprotocol.com/testimonials-1:
71
Multiple sclerosis, 7 Rheumatoid arthritis, 7 Atopic dermatitis, 4
Myasthenia gravis, 3 Vitiligo, 3 Psoriasis, 2 Neuromyelitis Optica
(NMO) or Devic's disease, 2 Lupus, 2 Lyme disease, 2 Sjogren's
syndrome, and one each for Spongiotic dermatitis, Fibromyalgia,
Alopecia, Schleroderma, Sjogren's syndrome, Psoriatic arthritis,
Idiopathic thrombocytopenic purpura, Type 1 diabetes (https:// www.coimbraprotocol.com/single-post/2018/08/01/valerio- marinaro-type-1-diabetes), Autoimmune polyneuropathy, Ichtyosis and Crohn's disease.
The
Coimbra protocol involves vitamin D3 supplementation, with a low
calcium, high water, diet (and probably vitamin K2 and attention to
other nutrients) in order to attain much higher than natural
25-hydroxyvitamin D levels, such as well above 100 ng/mL (250
nmol/L). This is done with medical monitoring of parathyroid
hormone and calcium levels: https:// www.mdpi.com/2072-6643/14/8/1575 and https:// www.tandfonline.com/doi/full/10.4161/derm.24808.
In addition, the Batcheller Protocol https:// vitamindstopscovid.info/06-adv/#pb, http:// www.clusterheadaches.com,
which is essentially the same as the Coimbra Protocol, successfully
suppresses both cluster headaches and migraines in thousands of
people. This was developed not by a doctor, or conventional
researcher, but by a retired U.S. Navy fighter pilot with a chemistry
degree.
Both
low 25-hydroxyvitamin D and absence of helminths greatly increase the
proclivity to the indiscriminate cell destroying immune responses which
are primarily evolved to tackle multicellular parasites, including
helminths. Ordinary adaptive immune responses (antibodies and
macrophages) evolved to deal with cancer cells, bacteria, yeast, fungi
and viruses. However, they work on individual cells and viruses
and are ineffective against multicellular parasites which have thick
layers or protective cells.
Indiscriminate
cell-destroying immune responses have evolved to tackle such
parasites. For instance eosinophils - the suicide bombers of the
immune system - arrive on the scene, disintegrate and release the
contents of the vacuoles which contain enzymes which destroy DNA, RNA
and proteins. Other type of immune cells, such as Th1 regulatory
lymphocytes, control the activities of these cell-destroying immune
cells, which kill host and parasite cells indiscriminately, by emitting
cytokines (short-distance immune system signaling molecules) which up-
or down-regulate the activities of eosinophils and the like.
"Inflammation"
has a general meaning of recruiting immune responses, but also a
particular meaning of unhealthy, self-destructive, indiscriminate
cell-destroying immune responses - from which you and many other people
suffer (along with our dewormed and often low-25-hydroxyvitamin D
companion animals).
Helminths
long ago (in mammalian or perhaps earlier vertebrate evolution) evolved
to exude one or more compounds which down-modulate these inflammatory
immune responses which target them. The response of the
hosts - our ancestors going back well before the evolution of humans
and probably primates in general - was to evolve stronger
indiscriminate cell-destroying immune responses, in the expectation
that these would be down-modulated by ubiquitous helminth
infections. Now we are all de-wormed, in general, humans
have excessively strong, self-destructive, inflammatory, indiscriminate
cell destroying immune responses. There is a great deal of
individual genetic variation in this, so those with persistent
inflammatory problems have probably inherited genetic patterns which
predispose them to this.
To
make matters much worse, most people have only a fraction of the 50
ng/mL 125 nmol/L of the circulating 25-hydroxyvitamin D their immune
systems need to function properly. This is needed for individual
immune cells (of many types) intracrine and paracrine signaling
systems, which communicate within each cell, and to nearby cells,
respectively, information the cells need in order to respond to their
changing circumstances.
As
far as I know, there are tutorial introductions to 25-hydroxyvitamin D
>>> calcitriol (1,25-dihydroxyvitamin D) intracrine and
paracrine signaling systems in the peer-reviewed
literature. Most doctors and immunologists have never
heard of these, yet they are crucial to the ability of the immune
system to work properly - and in most people today, they cannot work
properly due to low 25-hydroxyvitamin D levels. I wrote an
introduction at the start of: https:// vitamindstopscovid.info/00-evi/, based on a more detailed one at: https:// vitamindstopscovid.info/02-intracrine/.
Proper
operation of this intracrine signaling system is required for to enable
Th1 regulatory lymphocytes to transition from their pro-inflammatory
startup program to their anti-inflammatory shutdown program when they
detect the conditions to do so (a high level of a complement
protein). See Chauss et al. 2021 https:// www.nature.com/articles/s41590-021-01080-3 summarized at https:// vitamindstopscovid.info/00-evi/#chauss regarding
Th1 regulatory lymphocytes from the lungs of hospitalized COVID-19
patients failing to transition from their pro-inflammatory start-up
program to their anti-inflammatory shutdown program, despite detecting
the condition to do so. This failure of the Th1 cell's 25(OH)D
based intracrine signaling system was due primarily or wholly to
inadequate supplies of 25(OH)D.
References
#Quraishi-2014
These are four of the numerous articles concerning the D2 compounds being inferior to the D3 compounds.
#Houghton-2006
The case against ergocalciferol (vitamin D2) as a vitamin supplement
Lisa A
Houghton and Reinhold Vieth
American Journal of Clinical Nutrition
2006;84:694–7
doi.org/10.1093/ajcn/84.4.694
#Jones-2014
25(OH)D2 Half-Life Is Shorter Than 25(OH)D3 Half-Life and Is Influenced by DBP Concentration and Genotype
K. S.
Jones et al.
Journal of Clinical Endocrinology & Metabolism
2014-09-01
doi.org/10.1210/jc.2014-1714
#Nasim-2019
Efficacy of Vitamin D3 versus Vitamin D2 in deficient and insufficient patients: An open-label, randomized controlled trial
Bina
Nasim, Hana Al Sughaiyer, Samia Abdul Rahman, Rubina B. Inamdar, Razan Chakaki and Suha Abuhatab
Ibnosina Journal of Medicine and Biomedical Sciences
2019; 11(02): 57-61
doi.org/10.4103/ijmbs.ijmbs_8_19
This article reports that D3 calcitriol affects more and somewhat different genes than D2 calcitriol.
#Durant-2022
Vitamins
D2 and D3 Have Overlapping But Different Effects on the Human Immune
System Revealed Through Analysis of the Blood Transcriptome
Louise R
Durrant et al.
Frontiers of Immunology
2022-02-24
doi.org/10.3389/fimmu.2022.790444
#Hirsch-2010
#Miyauchi-2016
Determining
an Effective UV Radiation Exposure Time for Vitamin D Synthesis in the
Skin Without Risk to Health: Simplified Estimations from UV Observations
Masaatsu
Miyauchi and Hideaki Nakajima
Photochemistry and Photobiology
2016-10-18
onlinelibrary.wiley.com/doi/10.1111/php.12651
#Kimball-2020
#IOM-2011
Dietary Reference Intakes for Calcium and Vitamin D
Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium
Editors: A Catharine Ross, Christine L Taylor, Ann L Yaktine, and Heather B Del Valle.
National Academies Press
2011
www.ncbi.nlm.nih.gov/books/NBK56070/
#Veugelers-2014
A Statistical Error in the Estimation of the Recommended Dietary Allowance for Vitamin D
Paul J.
Veugelers and John Paul Ekwaru
Nutrients
2014-10-20
www.mdpi.com/2072-6643/6/10/4472
#Heaney-2015
Letter to
Veugelers, P.J. and Ekwaru, J.P., A Statistical Error in the Estimation
of the Recommended Dietary Allowance for Vitamin D
Robert
Heaney, Cedric Garland, Carole Baggerly, Christine French and Edward Gorham
Nutrients
2015-03-10
www.mdpi.com/2072-6643/7/3/1688
#WHO-2010
#WHO-2012
#Roizen-2019
#Elkhwanky-2020
#Zhu-2021
High Fat Diet and High Cholesterol
Diet Reduce Hepatic Vitamin D-25-Hydroxylase Expression and
Serum 25-Hydroxyvitamin D3 Level through Elevating
Circulating Cholesterol, Glucose, and Insulin Levels
Tengfei
Zhu et al.
Molecular Nutrition and Food Research
2021-08-27
onlinelibrary.wiley.com/doi/full/10.1002/mnfr.202100220
#Ekwaru-2014
The Importance of Body Weight
for the Dose Response Relationship of Oral Vitamin D
Supplementation and Serum 25-Hydroxyvitamin D in Healthy
Volunteers
John Paul Ekwaru, Jennifer D. Zwicker, Michael F.
Holick, Edward Giovannucci and Paul J. Veugelers.
PLoS One
2014-11-05
journals.plos.org/plosone/article?id=10.1371/journal.pone.0111265
#Wimalawansa-2022
Rapidly Increasing Serum
25(OH)D Boosts the Immune System, against Infections - Sepsis
and COVID-19
Sunil J.
Wimalawansa
Nutrients
2022-07-21
www.mdpi.com/2072-6643/14/14/2997
#Afshar-2020
Suggested role of Vitamin D
supplementation in COVID-19 severity
The authors are directors at Iranian Hospital Dubai, Dubai, UAE:
Parviz
Afshar, Hospital Director, Mohammad Ghaffaripour, ICU
Director and Hamid Sajjadi, Neuro-Ophthalmology Director.
Journal of Contemporary Medical Sciences Vol 6 No 4 (2020):
July-August 2020
2020-08-26
www.jocms.org/index.php/jcms/article/view/822
#Holick-2011
Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline
Michael
F. Holick, Neil C. Binkley, Heike A. Bischoff-Ferrari, Catherine M.
Gordon, David A. Hanley, Robert P. Heaney, M. Hassan Murad, Connie M.
Weaver
The Journal of Clinical Endocrinology & Metabolism, Volume 96, Issue 7, 2011-07-01
doi.org/10.1210/jc.2011-0385
#Luxwolda-2012
Traditionally living populations in East Africa have a mean serum 25-hydroxyvitamin D concentration of 115 nmol/L (46 ng/mL)
Martine F
Luxwolda, Remko S Kuipers, Ido P Kema, D A Janneke Dijck-Brouwer and Frits A J Muskiet
British Journal of Nutrition
2012-01-23
doi.org/10.1017/S0007114511007161
#Tebben-2015
Vitamin D-Mediated Hypercalcemia: Mechanisms, Diagnosis, and Treatment
Peter J.
Tebben, Ravinder J. Singh, and Rajiv Kumar
Endocrine Reviews
2016-09-02
doi.org/10.1210/er.2016-1070
#McCullough-2019
#Kamphius-2014
Calcium
and Vitamin D in Sarcoidosis: Is Supplementation Safe?
Lieke S Kamphuis, Femke Bonte-Mineur, Jan A
van Laar, P Martin van Hagen, Paul L van Daele
Journal of Bone and Mineral Research 2014-04-18
doi.org/10.1002/jbmr.2262
(Paywalled.)
sci-hub.se/10.1002/jbmr.2262
#Hewison-2009
Vitamin D-Mediated Hypercalcemia in Lymphoma: Evidence for Hormone Production by Tumor-Adjacent Macrophages
Martin
Hewison, Vitaly Kantorovich, Harley R Liker, Andre J Van Herle, Pejman Cohan, Daniel Zehnder and John S Adams
Journal of Bone and Mineral Research
2009-12-02
doi.org/10.1359/jbmr.2003.18.3.579
#Sternlicht-2015
Hypercalcemia of malignancy and new treatment options
Hillel
Sternlicht and Ilya G Glezerman
Therapeutics and Clinical Risk Management
2015-10-23
doi.org/10.2147/TCRM.S83681
#Fuleihan-2023
Treatment of Hypercalcemia of Malignancy in Adults: An Endocrine Society Clinical Practice Guideline
Ghada El-Hajj
Fuleihan et al, for the Endocrine Society
The Journal of Clinical Endocrinology & Metabolism, Volume 108, Issue 3, March
2023
https://doi.org/10.1210/clinem/dgac621
#Israel-2020
#Darling-2020
Very high prevalence of 25-hydroxyvitamin D deficiency in 6433 UK South Asian adults: analysis of the UK Biobank Cohort
Andrea L.
Darling, David J. Blackbourn, Kourosh R. Ahmadi and Susan A. Lanham-New.
British Journal of Nutrition
2020-07-22
doi.org/10.1017/S0007114520002779
#Sutherland-2020
Differences and determinants of vitamin D deficiency among UK biobank participants: A cross-ethnic and socioeconomic study
Joshua P.
Sutherland, Ang Zhou, Matthew J. Leach and Elina Hypponen
Clinical Nutrition
2020-11-17
doi.org/10.1016/j.clnu.2020.11.019
#W
Appendix 1 - Rare adverse reactions
I
regard these first two reports of heart aryhtymias in response to
healthy vitamin D3 supplementation as most likely genuine, though the
third observational article lacks detail, is at odds with a meta-analysis and can't necessarily
disentangle reverse causation such as those with general ill-health
being motivated to supplement higher amounts of vitamin D3.
The first report of heart palpitations I knew of was from a friend, in her 60s, who
found, by experimentation, that her vitamin D3 supplementation (I don't
recall the amount, but it was less than 5000 IU/day) seemed to
be causing her heart palpitations. I can't attest to her
general health, which is not perfect. I think she drank
caffeinated tea / coffee. I have no idea what else she was supplementing.
The second report was from another friend, in his 60s, who I have
known
for decades. He did
not use caffeine, and he found that with at least two forms of vitamin
D3, ca. 5000 IU a day, that he developed a pattern of a racing heart,
at least at some times in the day or evening. He did not supplement calcium
and I recall that he did supplement magnesium and fish oil. He
went off vitamin D3 and on again,
and perhaps a third time, and I recall that he tried a different type
of capsule. He found consistently, in the second or
third rounds of resuming vitamin D3 supplementation that the symptoms
reappeared within a day or so.
#2024-10-17 update:
In the printed version, I wrote:
I have no idea what mechanisms
might
explain this, but the Deva Boone MD report below is probably pertinent.
Today
I spoke with my friend again. He told me that after the events of
early 2023,reported above, he was having heart arrhythmias even without
supplemental vitamin D3. He was subsequently diagnosed with supraventricular tachycardia (SVT), though I am not sure which of the 8 types the Mayo Clinic lists: www.mayoclinic.org/.../supraventricular-tachycardia/...
He
now takes a blood pressure drug and a second drug to combat the SVT
itself. I guess he is not supplementing vitamin D3, and his
symptoms have fluctuated, becoming worse in the last week or so.
A Google Scholar search for
"supraventricular tachycardia" "Vitamin D" turned up lots of
articles on SVT being associated with, and so presumably in part caused
by, low 25-hydroxyvitamin
D and/or hypocalcemia. The only potentially interesting article I
found reference to which might concern higher 25(OH)D levels
precipitating SVT was a 2015 article "Two cases of cardiac sarcoidosis
in pregnant women with supraventricular arrhythmia" http://www.cvja.co.za/...50.html
The
only mention of vitamin D in this article is that one of the women was
given unspecified amounts of supplemental vitamin D and calcium after
giving birth, with this continuing to 10 months later with her symptoms
reducing. There was no other mention of calcium, so the suspected
sarcoidosis may not have caused hypercalcemia.
Cardiac sarcoidosis can be a very
serious matter, including resulting in sudden death.
Generally, I would expect high 25(OH)D to protect against the
development of sarcoidosis or any other granulomatous disorder, and for
this higher, healthier, level to reduce the the immune system
dysfunction which causes or at least facilitates sarcoidosis.
There are plenty of articles concerning "supraventricular tachycardia" sarcoidosis.
IF the tachycardia was caused or worsened by hypercalcemia, and IF
already already developed sarcoidosis resulted in higher calcium levels
when vitamin D3 is supplemented at ca. 5000 IU/day rates, THEN we might
have an explanation for high 25(OH)D - or at least higher than before
vitamin D3 supplementation - precipitating heart arrhythmias, due to
more 25(OH)D being available for conversion to pathologically
circulating calcitriol.
This extensive review article:
makes it clear that hypercalcemia raises the risk of heart arrhythmias.
So, perhaps vitamin D3
supplementation with already incident sarcoidosis (perhaps anywhere in
the body, not specifically the heart) could, in principle,
increase the risk of heart arrhythmias due to the greater supply of
25(OH)D to the granulomatous lesions enabling them to produce even more
calcitriol. This would be despite this higher 25(OH)D being
generally healthy, likely to reduce the risk of development of
sarcoidisis, and in some or many cases, actually contributing to the
suppression of the sarcoidosis.
If so, it does not necessarily
follow that all vitamin D3 supplementation as suggested above be done
only under medical supervision, even if we ignore the argument below
about the rare serious risk being justified by the very substantial,
very high probability, significant improvement in health such
supplementation brings.
For instance, if vitamin D3
supplementation exacerbates a serious condition to the point of
producing obvious symptoms, then as long as those symptoms do not cause
lasting harm, this is arguably a good result, since the obvious
symptoms will generally result in the person seeking medical treatment
earlier than if their symptoms developed more gradually.
I have been meaning to ask the NISH list vitamin D researchers about this, but have not yet done so.
This section ends with an argument for
robust vitamin D3 supplementation of the whole population, without
medical monitoring, as described above, despite this probably leading
to a small number of potentially serious adverse reactions.
To insist on blood tests and medical monitoring would continue to
condemn the great majority of the population of all countries to weak
and sometime debilitating immune dysfunction for their entire lives.
The same logic applies in everyday activities: We routinely
undertake on-average healthy activities such as walking or running in
urban areas for exercise, or driving to medical appointments, despite
the small, but non-zero risk we will be injured or killed in a traffic
accident.
It is important to be open to
indications of adverse reactions to vitamin D3 supplementation which
have not yet been properly recognized by researchers or documented in
the peer-reviewed literature. Extensive long-term research such as that in the psychiatric hospital mentioned above (#McCullough-2019), may not detect subtle and relatively rare adverse reactions.
Here is an example of how such
reactions may fly under the mainstream medical radar, while being mentioned
in apparently substantial non-peer-reviewed web pages and the like.
- www.devaboone.com/post/vitamin-d-part-2-shannon-s-story
2020 patient report by Deva Boone, MD, of Phoenix AZ, who specializes
in parathyroid diseases. A 38 year old, previously healthy, woman
lost weight and suffered difficulty speaking, heart palpitations, heart
rates of 90 BPM even in bed, anxiety and cognitive deficits which Dr
Boone, but not other doctors, attributed to "moderately elevated
calcium levels up to 11.2 mg/dL (normal for
her age would be up to 10.2 mg/dl)". The patient had been taking
125 micrograms (5000 IU) vitamin D3 a day, without supplemental
calcium, for seven years, as advised by a doctor who diagnosed her with
mild osteopenia. Her parathyroid hormone levels did not raise
concern.
"Most patients with high
calcium develop fatigue and body aches, and just generally feel bad.
They may develop insomnia and palpitations, a feeling like the heart is
racing. Some have more severe neurologic symptoms like muscle weakness
and problems with balance, and some have psychiatric symptoms like
depression and anxiety."
Dr Boone attests that "vitamin D is a steroid hormone" and that the
patient's 25(OH)D level of 79 ng/mL was within the 70 to 100 ng/mL
range in which she had previously observed toxicity. Six months
after stopping vitamin D3 supplementation her level dropped into the
50s.
(This
seems like a long time - I thought the half-life of circulating 25(OH)D
was weeks at such levels, but that may be before long-term tissue
stores have developed.)
"As it fell, her calcium level gradually started to normalize, and her symptoms slowly resolved. . . . 'It’s a hormone!' she exclaimed. 'If I had to take ‘Hormone D’, I would have questioned my doctor about why I needed it.' "
- jeffchen.dev/posts/Vitamin-D-And-Heart-Palpitations/ Self report, prompted by the above, by a software engineer and athlete.
-
A 2011 conference presentation, which while not peer reviewed,
is the product of formal research with a large number of subjects:
"Abstract 14699: Vitamin D Excess Is Significantly Associated with Risk
of Atrial Fibrillation" Megan B. Smith et al. www.ahajournals.org/doi/abs/10.1161/circ.124.suppl_21.A14699.
Contrary to this conference presentation, a meta-analysis: The relationship between vitamin D and risk of atrial fibrillation: a dose-response analysis of observational studies, Xiao Liu et al. Nutrition Journal 2019-11-14 doi.org/10.1186/s12937-019-0485-8, reports that higher 25-hydroxyvitamin D levels were associated with decreased risk of atrial fibrillation.
Generally healthy supplemental vitamin D3
quantities, such as those recommended above, reduce the risk of
atrial fibrillation, which is a common and potentially serious form of
heart arrhythmia, in the general population. However, perhaps, in
some
individuals, similarly and generally healthy vitamin D3 supplemental
quantities increase the risk, or the risk of some other form of heart
arrhythmias.
One response to cases such as this would be to insist that everyone who
supplements vitamin D in quantities sufficient to attain at least the
50 ng/mL circulating vitamin D3 do so with regular 25(OH)D, PTH and
calcium blood tests and medical monitoring. However, this is
rarely possible in rich developed countries even for adults of working
age. To insist on such expensive protection against rare
individuals who would suffer hypercalcemia would deny the vast majority
of the population, of all ages,
in all countries, the ability to have a fully functioning immune system.
The patient described above suffered serious and potentially deadly
symptoms which were directly obvious without the need for medical examination or tests. This led to medical
intervention, and resolved completely with lower but still healthy
25(OH)D levels. By supplementing vitamin D3 substantially, she presumably avoided developing osteoporosis at
an early age. Assuming she continues to take smaller amounts of
vitamin D3, since her early thirties and for the rest of her life she
was, and will remain, at much lower risk of numerous diseases, not
least cancer and dementia, than she would have been without any
supplementary vitamin D3.
People with poorly functioning immune systems - or crippled immune
systems for those with 25(OH)D levels below 10 ng/mL (25 ng/mL) - as
are 43 to 65% of UK 45 to 69 year olds of Bangladeshi, Indian and
Pakistani ethnicity (#Darling-2020) - are
not just a threat to their own wellbeing, but are a greater risk to the
health of others through harboring infectious diseases and antibiotic
resistant bacteria and through poorer health when driving. Women of childbearing age with such low
levels are at much greater risk of pre-eclampsia, preterm birth, still
birth and of their surviving children suffering profound neurological
deficits.









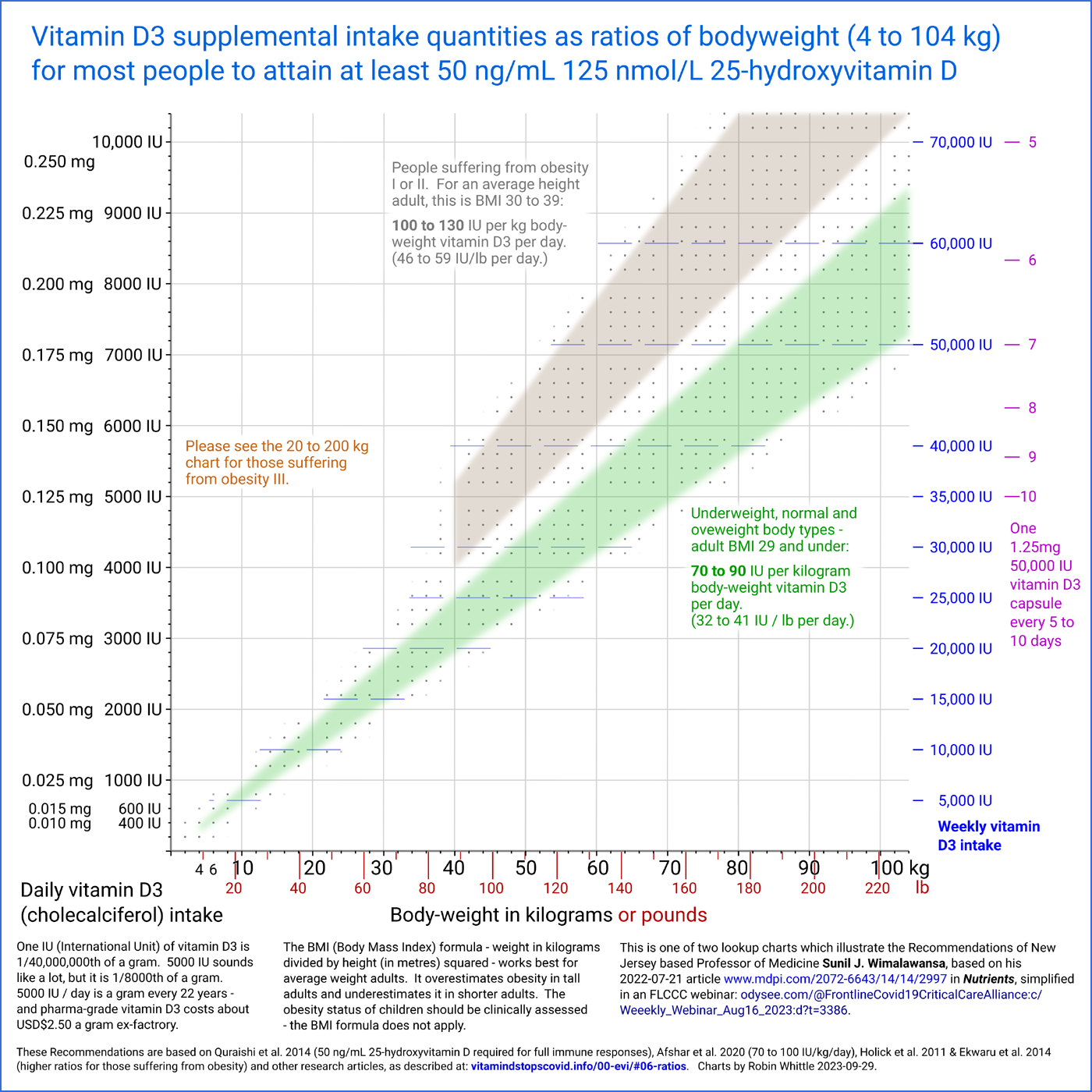{kind=link}
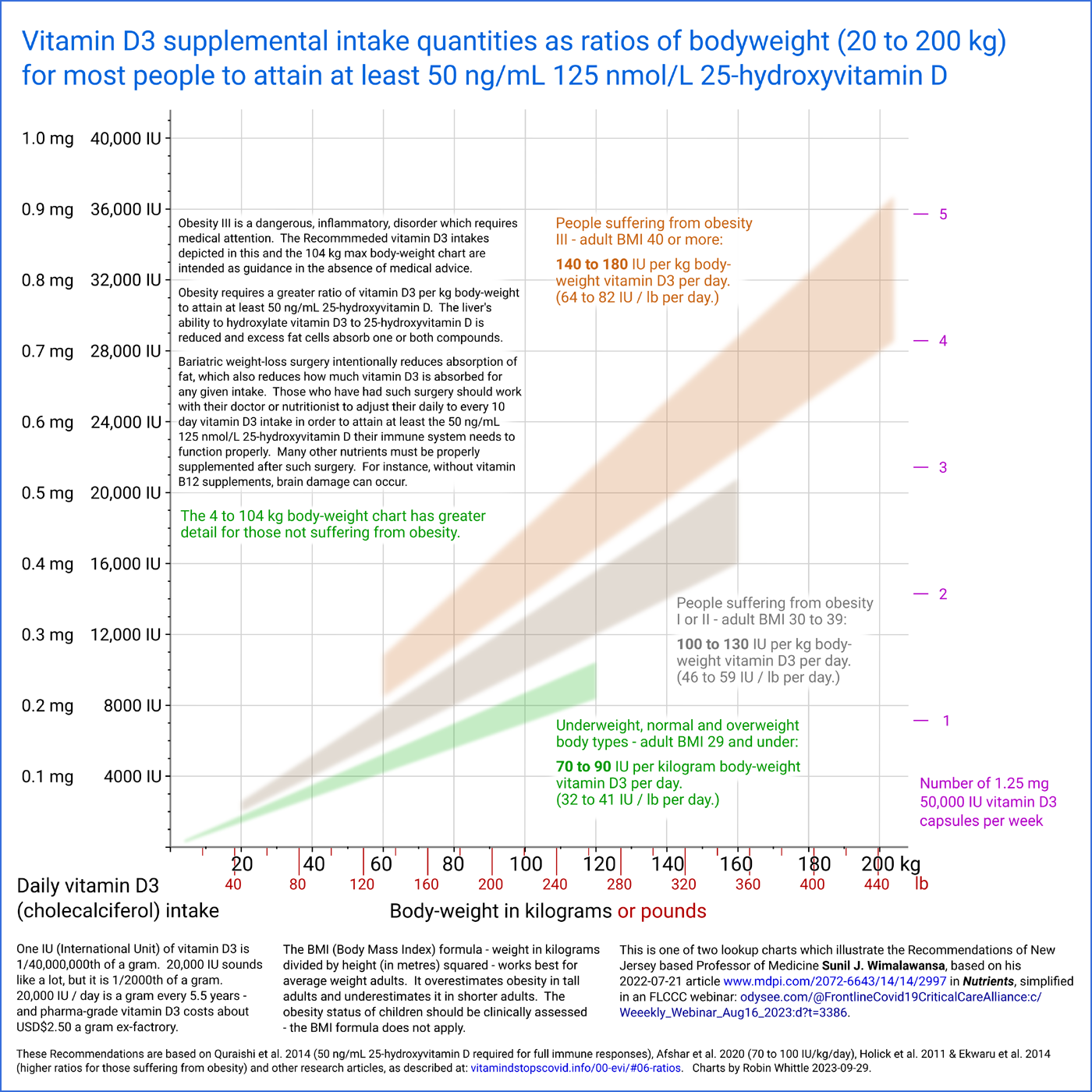{kind=link}